

IMPORTANT SAFETY INFORMATION for Omvoh (mirikizumab-mrkz)
Warning:
CONTRAINDICATIONS - Omvoh is contraindicated in patients with a history of serious hypersensitivity reaction to mirikizumab-mrkz or any of the excipients.
WARNINGS AND PRECAUTIONS
Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylaxis during intravenous infusion, have been reported with Omvoh administration. Infusion-related hypersensitivity reactions, including mucocutaneous erythema and pruritus, were reported during induction. If a severe hypersensitivity reaction occurs, discontinue Omvoh immediately and initiate appropriate treatment.
Infections
Omvoh may increase the risk of infection. Do not initiate treatment with Omvoh in patients with a clinically important active infection until the infection resolves or is adequately treated. In patients with a chronic infection or a history of recurrent infection, consider the risks and benefits prior to prescribing Omvoh. Instruct patients to seek medical advice if signs or symptoms of clinically important acute or chronic infection occur. If a serious infection develops or an infection is not responding to standard therapy, monitor the patient closely and do not administer Omvoh until the infection resolves.
Tuberculosis
Evaluate patients for tuberculosis (TB) infection prior to initiating treatment with Omvoh. Do not administer Omvoh to patients with active TB infection. Initiate treatment of latent TB prior to administering Omvoh. Consider anti-TB therapy prior to initiation of Omvoh in patients with a history of latent or active TB in whom an adequate course of treatment cannot be confirmed. Monitor patients for signs and symptoms of active TB during and after Omvoh treatment. In clinical trials, subjects were excluded if they had evidence of active TB, a history of active TB, or were diagnosed with latent TB at screening.
Hepatotoxicity
Drug-induced liver injury in conjunction with pruritus was reported in a clinical trial subject following a longer than recommended induction regimen. Omvoh was discontinued. Liver test abnormalities eventually returned to baseline. Evaluate liver enzymes and bilirubin at baseline and for at least 24 weeks of treatment. Monitor thereafter according to routine patient management. Consider other treatment options in patients with evidence of liver cirrhosis. Prompt investigation of the cause of liver enzyme elevation is recommended to identify potential cases of drug-induced liver injury. Interrupt treatment if drug-induced liver injury is suspected, until this diagnosis is excluded. Instruct patients to seek immediate medical attention if they experience symptoms suggestive of hepatic dysfunction.
Immunizations
Avoid use of live vaccines in patients treated with Omvoh. Medications that interact with the immune system may increase the risk of infection following administration of live vaccines. Prior to initiating therapy, complete all age-appropriate vaccinations according to current immunization guidelines. No data are available on the response to live or non-live vaccines in patients treated with Omvoh.
ADVERSE REACTIONS
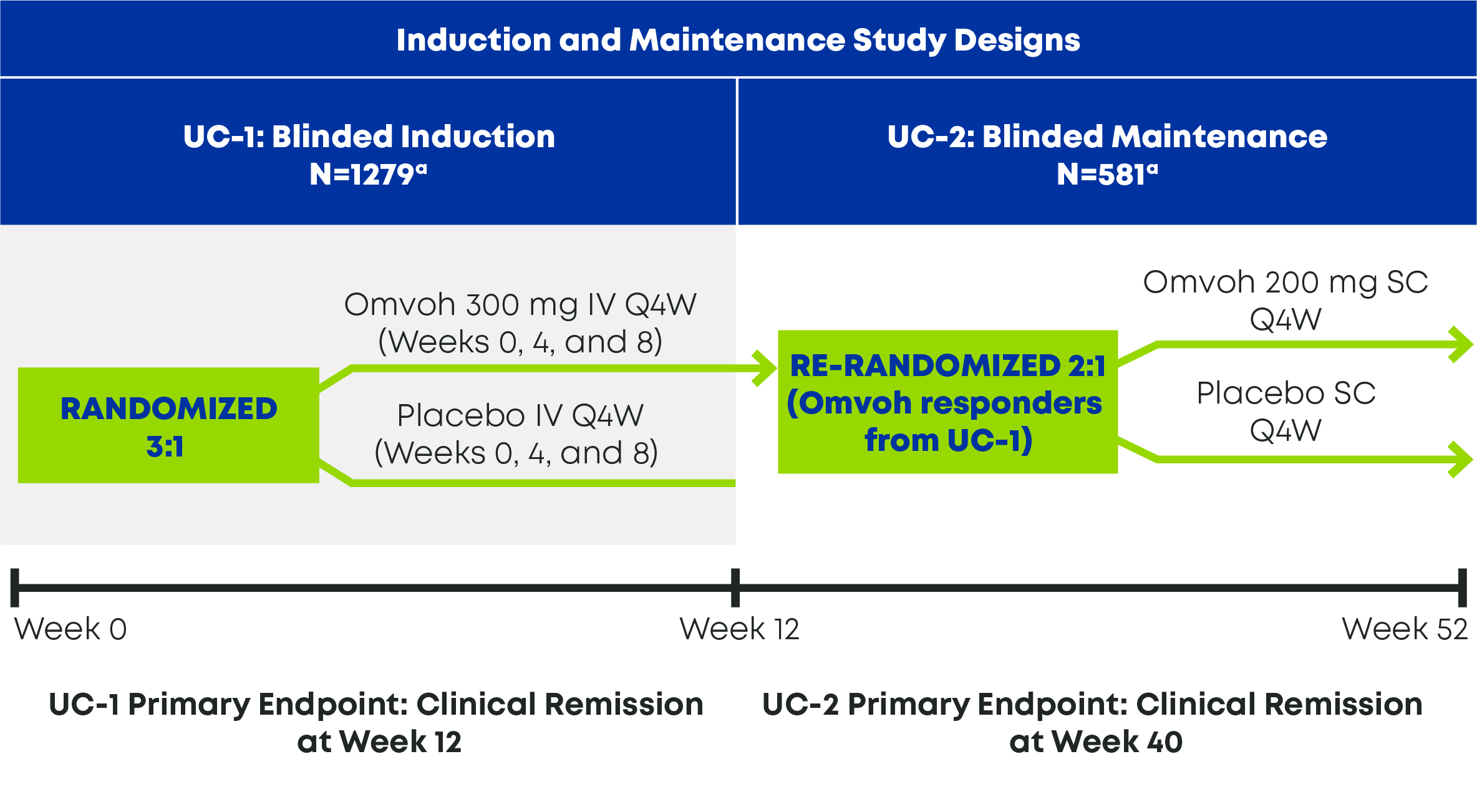
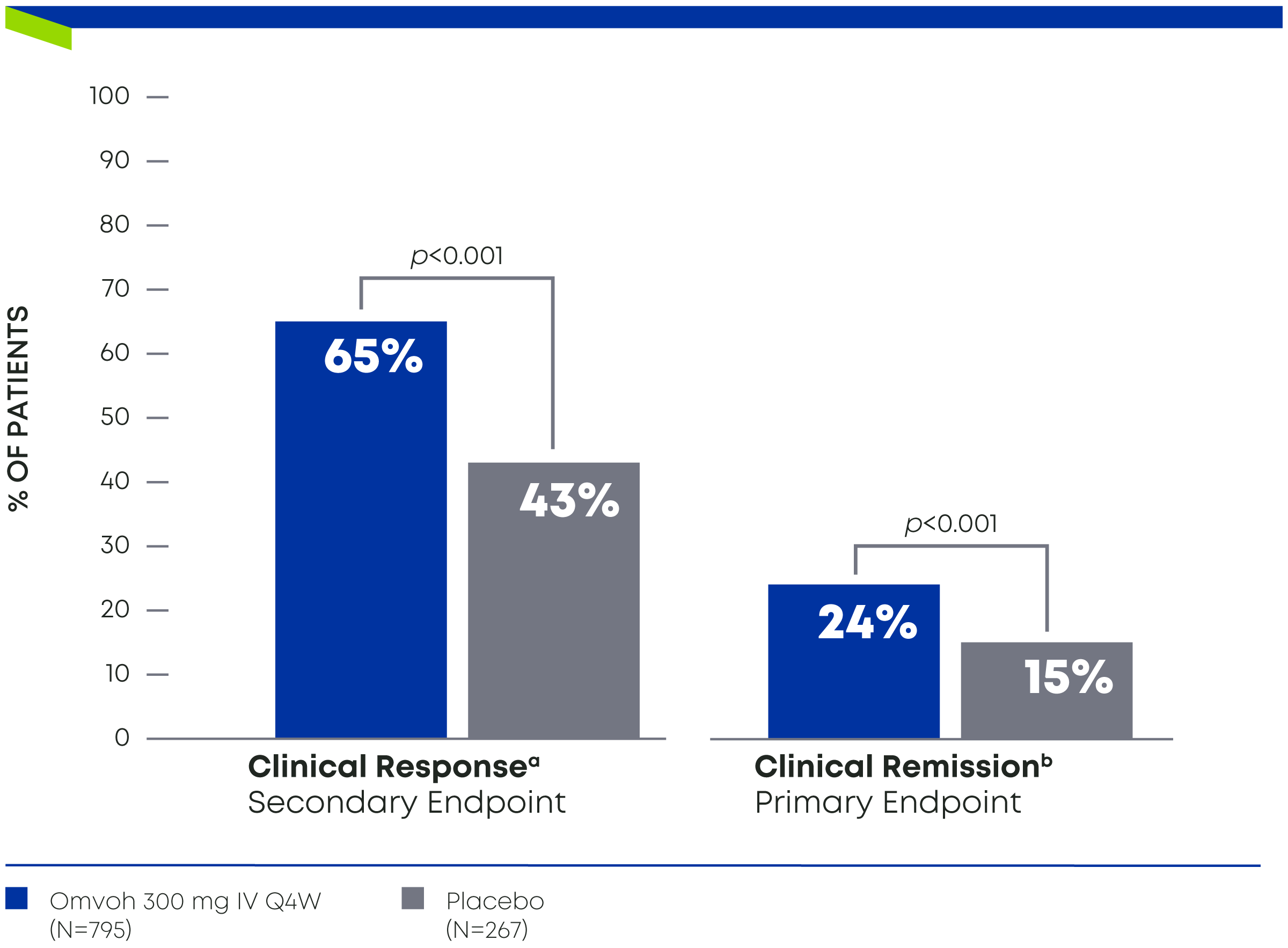
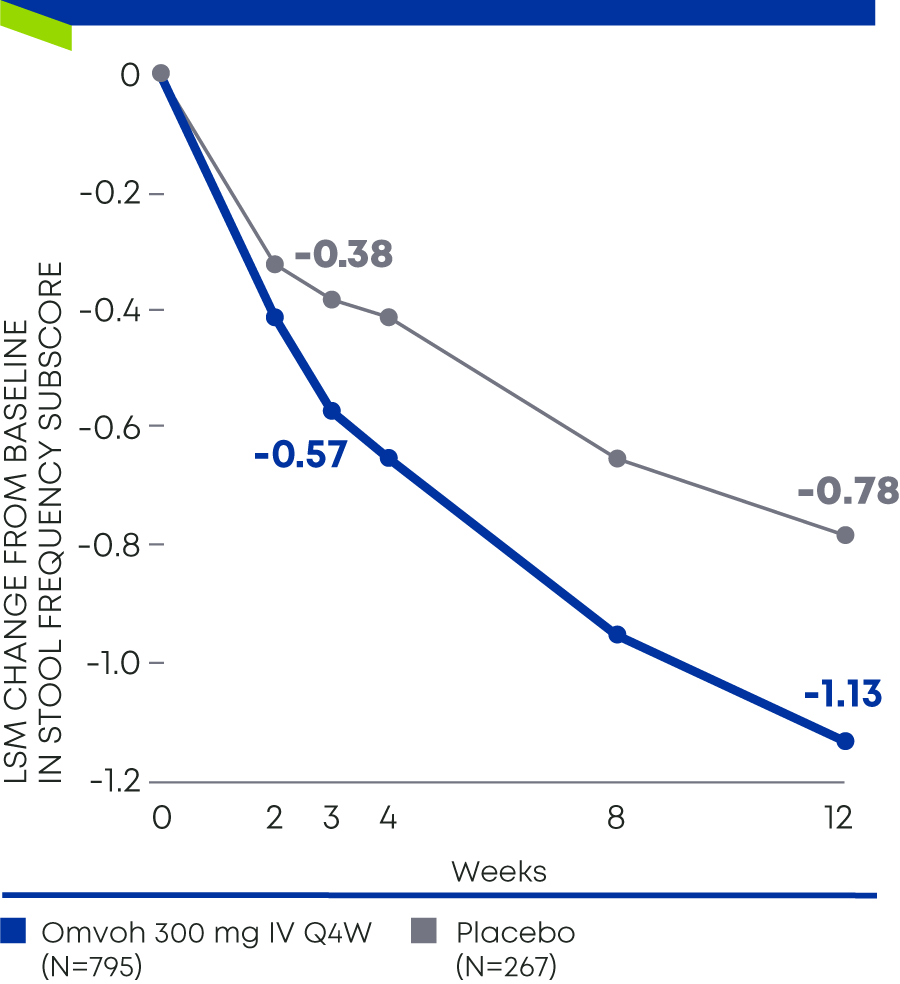
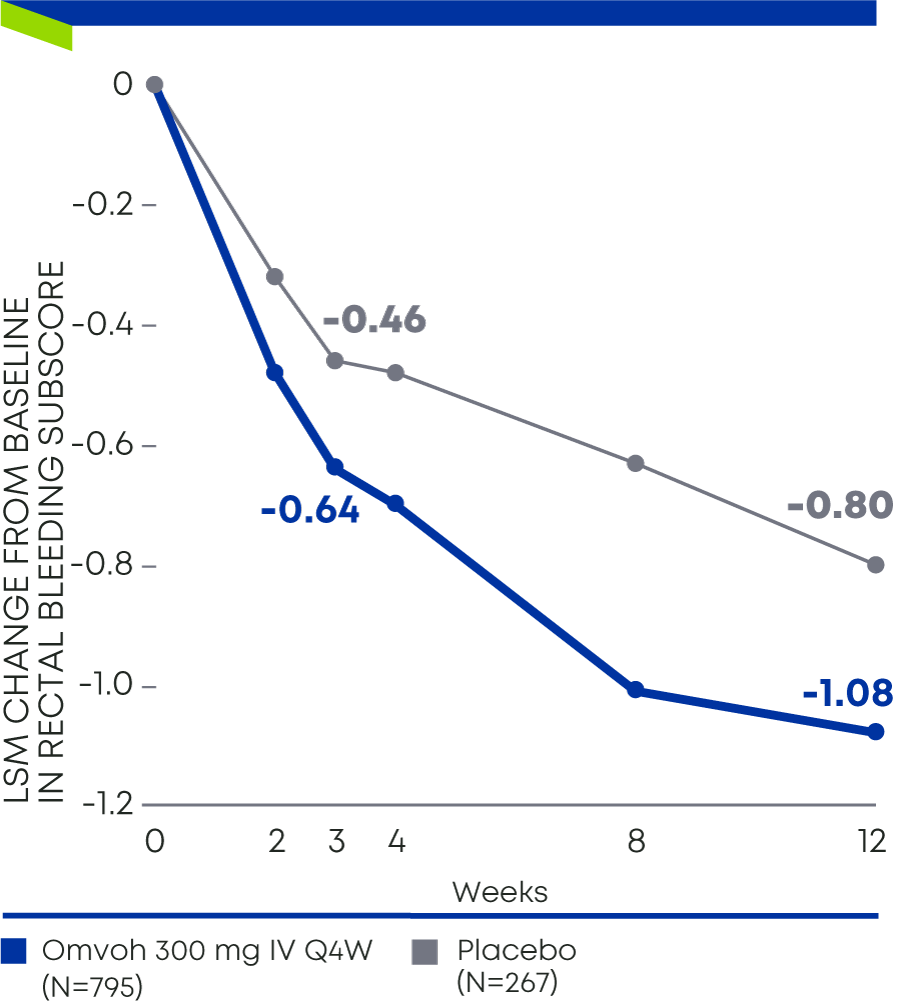
Most common adverse reactions associated with Omvoh (≥2% of subjects and at a higher frequency than placebo) in ulcerative colitis treatment are upper respiratory tract infections and arthralgia during the induction study (UC-1), and upper respiratory tract infections, injection site reactions, arthralgia, rash, headache, and herpes viral infection during the maintenance study (UC-2).
Most common adverse reactions associated with Omvoh in the Crohn’s disease study (CD-1) (≥5% of subjects and at a higher frequency than placebo) are upper respiratory tract infections, injection site reactions, headache, arthralgia, and elevated liver tests.
Omvoh injection is available as a 300mg/15 mL solution in a single-dose vial for intravenous infusion, and as a 100 mg/mL solution or a 200 mg/2 mL solution in a single dose prefilled pen or prefilled syringe for subcutaneous injection. Refer to the Prescribing Information for dosing information.
MR HCP ISI CD APP
Please see Prescribing Information and Medication Guide for Omvoh. Please see Instructions for Use included with the device.